







Treatment of legs veins with IPL
Treatment of legs veins with IPL and ND:yag Laser.
For many years various laser treatment systems have been used in the treatment of vascular injuries. Laser is a device that is made up of active media, including gases, liquids, or solids enclosed within a resonating chamber, bounded by a pair of smooth, parallel mirrors, some perfectly clear and others semi-transparent.
Einstein was first who suggested the basis for the controlled manipulation of light waves in 1917, but it was not until 1960 that the first laser was built (light amplification by stimulated emission of radiation), and some of the first applications were in the treatment of cutaneous vascular injuries. This gave rise to the argon laser, invented in 1960 by Maiman, which was a continuous emission laser with light wave lengths ranging between 488 and 514 nm.
Subsequently, in the mid-nineties the Photoderm (IPLS-intense pulsed light source) came about which used a high energy flash lamp system with a spectrum of variable wave lengths ranging from 515 to 1200 nm.
The most recent laser used in the treatment of blood vessels is the ND YAG pulsating at a length of 1.064 nm and called the Vasculight light, which emits energy up to 150j/cm2. This system is based on the deep penetration of these wave lengths in order to photocoagulate larger blood vessels (especially in the lower extremities), as reticulated varicose veins, essential and secondary telangiectasias, and, therefore, substituting for sclerotherapy. The light of the laser is absorbed in a selective way by chromophore (hemoglobin), generating heat above the point of coagulation and causing the re-absorption of the vascular walls.
As supposed, the pathologies that involve various veins are conditioned by the location and function of each–the network of deep veins and controlling a high percentage of the blood-return veins (approximately 80%)–and is associated with areas of vein insufficiency. The perforated veins suffer injuries at times in their valvular structures, losing the unidirectional nature of their flow, by which the incoming blood in the deep system flows to the superficial veins, dilating them and becoming varicose.

As is well known, the prevalence of vein pathology, in our environment, is extraordinarily elevated. This contributes a diversity of factors that are not congenital, but can be acquired in other ways, such as multiple pregnancies, injuries, standing for long periods of time, etc. From this point of view, the illnesses included in this category, as in other similar ones, show evidence of the strong presence of factors related to educational and cultural order.
The surface veins are dilated and twisted with defective valves. Commonly, this is a problem that involves the interior and exterior saphenous veins. The highest incidence of this appears at the age of 20 and is three times more frequent in women than in men because of the intervention of PRE factors related primarily to pregnancy, menopause, and genetics. This also is a consequence of deep thrombophlebitis with vein re-channeling.
Our objective is to evaluate the results obtained with the pulsating Photoderm and the Vasculight in the treatment of vein insufficiency in the lower extremities
Between October, 1998 and August, 1999, 125 patients were treated who had vein insufficiency in the lower extremities, all women between the ages of 26 and 45 with the Photoderm V/L system with Fitzpatrick 3 to 5 photo-types, using the following 550 and 570 filters. Later on in August, 1999 and September, 2002, treatment was continued with the Vasculight system, having a treatment group of 210 cases composed of which 97.24% were women and 2.76% were men between the ages of 20 and 70.
All cases involved spider veins, telangiectasias, reticular, and some with snaky veins. The parameters that were utilized for telangiectasias were low power, for the reticular we used 110 j/cm2 at a single pulse with a delay of 12 ms and for larger veins (greater than 6mm) we used 120 j/cm2 with a double pulse and a delay of 7 ms.
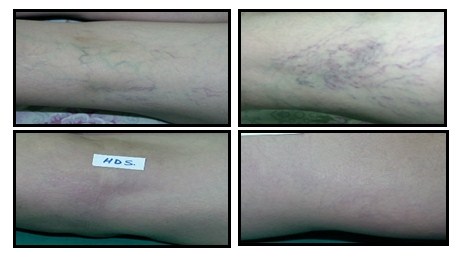
We obtained good results with Photoderm alone in telangiectasias. However, with the Vasculight the clinical improvement seen in the patients with vein insufficiency had been an average of 80 to 85%. Table 1. We only had two cases that left treatment because of pain related to the treatment.
The complications that developed after treatment were hyper-pigmentation which had a spontaneous resolution without consequences, and the hypo-pigmentation had lessened with the application of Puva therapy and exposure to sun over the next 6 months.
Table 1. Veins percentage clearance after treatment.
Lesion type # patients % clearance
Reticular veins 183 80
Telangiectasias 152 85
The therapy used for the treatment of vein insufficiency in the lower extremities with Vasculight, is an ambulatory treatment, requiring no convalescence other than avoiding exposure to the tanning effect of the sun during treatment. The improvement obtained in the first session had been on an average of 30% and by the third session there was a 70% improvement in symptoms from the first session, such as pain, edema in the feet, sensations of numbness, and changes in temperature.
Clínica Dermatológica y Cirugía Estética de Puebla
Clínica Láser Puebla
Cita de valoración + 52 (222) 243 65 05 y 243 77 40
Puebla, Pue. México www.laserpuebla.com info@laserpuebla.com
Tags: Cirugía Estetica Puebla, Clinica Dermatologica Puebla, costo tratamiento vasculight, dr. aristides arellano, inflamación de venas, Tratamiento para várices, Treatment of legs veins, vasculight, venas venas reticulares y telangiectacias
